Authors
More health systems than ever brought their managed care contracts into the Turquoise platform this year, which meant we spent a lot of time inside the digital equivalent of their filing cabinets. Awash in contracts, we wondered what we might find if we lent an inquisitive eye to healthcare administrators' most valuable bits of paper?
Among base agreements that predate modern care models (and the iPhone…), amendments layered like geological strata, and contracts that grew like weeds, what we found wasn’t a broken system—it was a busy one. This review reflects what we learned by gently, respectfully, opening those filing cabinets. It’s a portrait not of the entire industry, but of the patterns inside the contracts we ingested: age, length, layers, timelines, rate structures, and what they might reveal about healthcare administration as a whole.
So, grab a drink and your filing cabinet.
We’re going in.
A quick note on methodology
The observations in this blog are based on a large and diverse sample of managed care contracts ingested into the Turquoise Health platform over the past year. These documents span the majority of the US, care settings, provider types, and payer relationships, offering a wide lens into the contractual language and structures we encounter most often. This dataset, of course, does not include every payer<>provider agreement in the United States, nor is it intended to represent the complete national landscape of managed care contracting. This blog will not include any confidential, identifiable, or contractual information from any contract. Instead, the goal is to highlight recurring patterns, operational challenges, and structural themes we’ve observed across the market. We offer these insights as signals rather than definitive industry-wide benchmarks. It’ll be fun. We promise.
Drawer 1: The Sheer Quantity of Files
Observing tens of thousands of commercial contracts across the majority of the US, we can confidently say: Healthcare organizations are still buried in paperwork.
A typical health system brings between 1,000-5,000 contract files to the platform
Most health systems arrive with contracts that number in the thousands. This quantity isn't a bad thing—it’s a sign of a robustly operating health system. Instead, think of it as quantifying what the true “work” of contracting is: relationship management. Every single contract is a single payer<>provider relationship that demands vigilance and regular re-negotiation. Thousands of contracts represent decades of payer relationships, acquisitions, service-line expansions, and legacy agreements all with their own unique policies, fee schedules, stipulations, algorithms, and filing limits.
If you start to think about the practical applications of operating a business with thousands of contracts, even simple questions like “What is the filing limit for this payer?” or “Where are our current rates listed?” become operationally complex. High document volume means high cognitive load, and it’s one of the root causes of variation, denials, and avoidable friction both within a provider organization and as both providers and payers attempt to conduct business between themselves.
Drawer 2: The Age of the Paperwork
The median contract age is over 10 years old
The median contract in the platform is over a decade old, and many are far older. Keep in mind that the vast majority of these contracts have countless amendments made over the years of a maintained relationship. These are the base agreements a.k.a. the language those amendments build upon. (More on amendments in a bit)
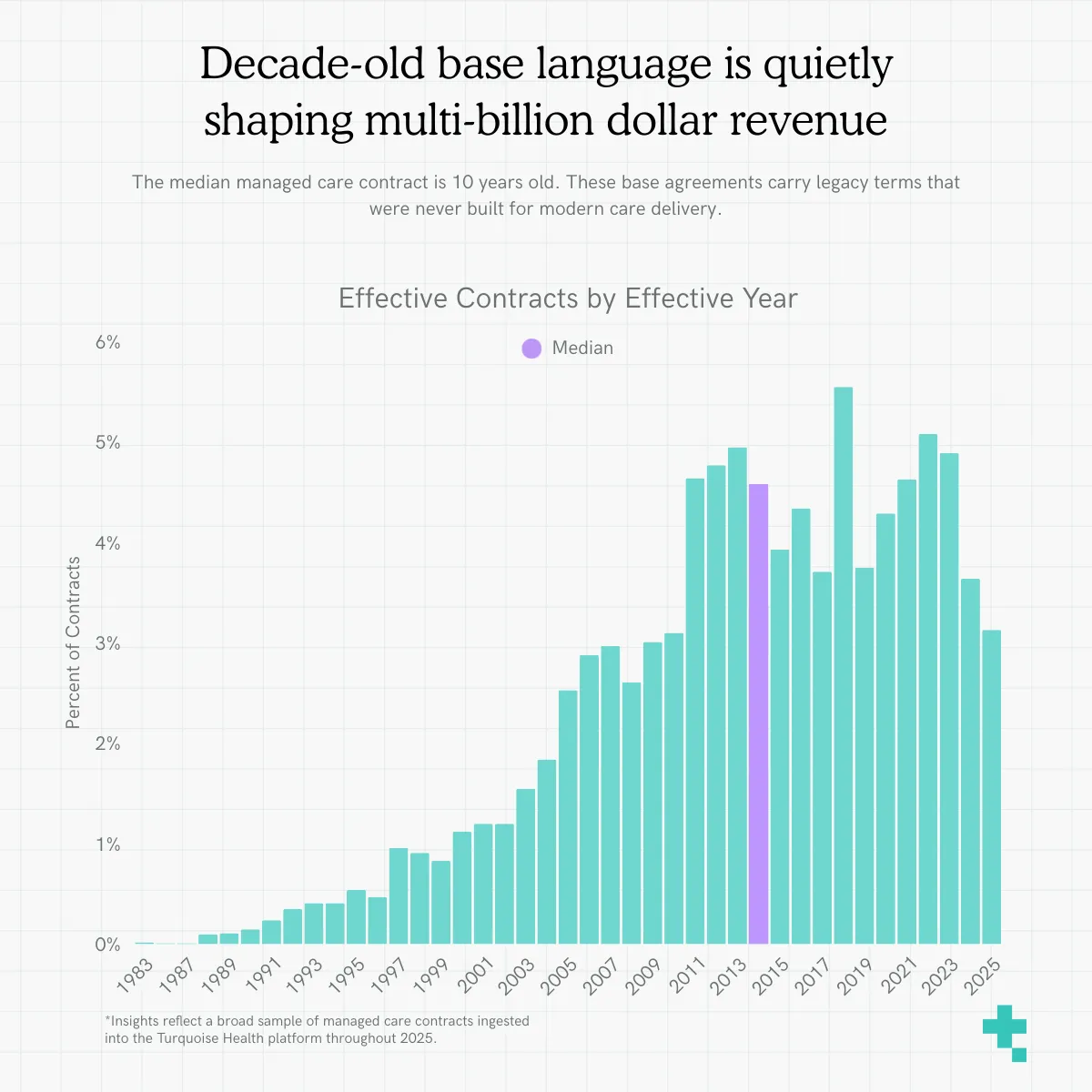
Instead, think of median contract age as an indicator of operational modernity. When base language is upwards of ten years old, reimbursement terms are often anchored to assumptions, definitions, and payment methodologies that no longer reflect today’s care models or cost structures. When contracts age without comprehensive repapering, outdated logic persists: legacy CMS references, archaic authorization language, and negotiated terms that never contemplated post-COVID population health, ambulatory trends, or site-neutrality shifts. Old documents don’t just feel stale; they quietly shape multi-billion-dollar revenue streams and stagnating ways of conducting business. (Dun, dun, dunnn)
Drawer 3: Layers Upon Layers of Amendments
Since 2008, more amendments have been created than base language
The legal equivalent of White-Out, amendments allow organizations to make minimal or substantial changes to their base business agreements. Amendments aren’t a problem, in many cases they’re the most efficient way to update a contract. However, it’s interesting to note a shift in the industry’s use of amendments.
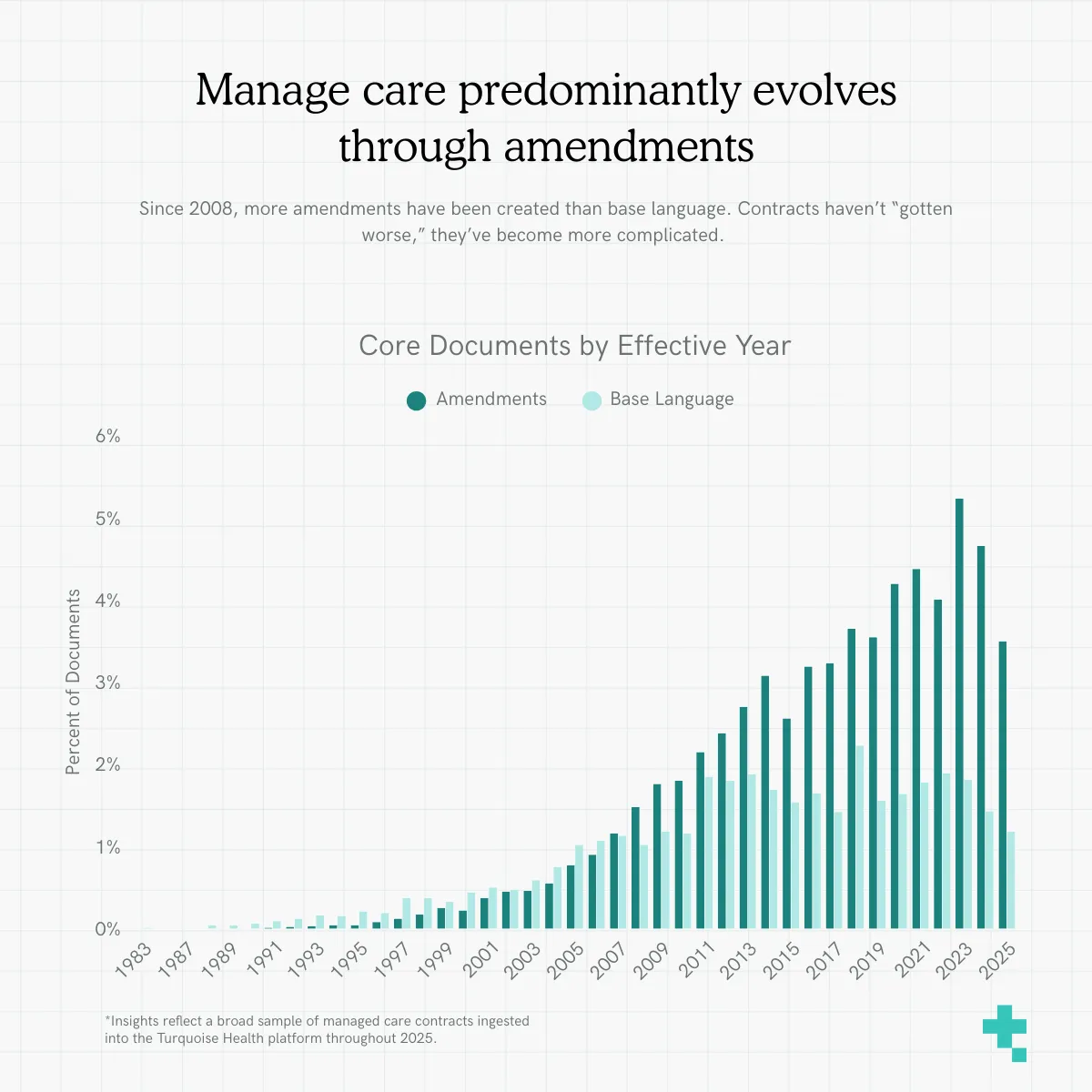
Looking at the effective dates of both base languages and amendments, we see the number of amendments has outpaced the creation of new base languages since 2008. This steady upward trend is notable: year-over-year, organizations are relying more heavily on amendments than full repapering. The past 10+ years of managed care contracting have been defined by this operational shift. Contracts haven’t “gotten worse,” they’ve become more complicated.
A few targeted amendments can be helpful, but a dozen or more creates a patchwork document full of superseded clauses, contradictory definitions, and legacy rate appendices. When payer policies evolve faster than base agreements are rewired, teams are left to interpret which clause “wins.”
Instead of repapering base language, which would decrease overall document complexity, the industry has predominantly spent the last fifteen years "modernizing" their agreements via amendments.
Drawer 4: The Size of Each Stack
Most base agreements ranged between 10-30 pages, while the majority of amendments are <10 pages
Breaking down the contracts within our platform, the distribution shows most base agreements land in the 10–30 page range, with amendments between 1-10 pages long.
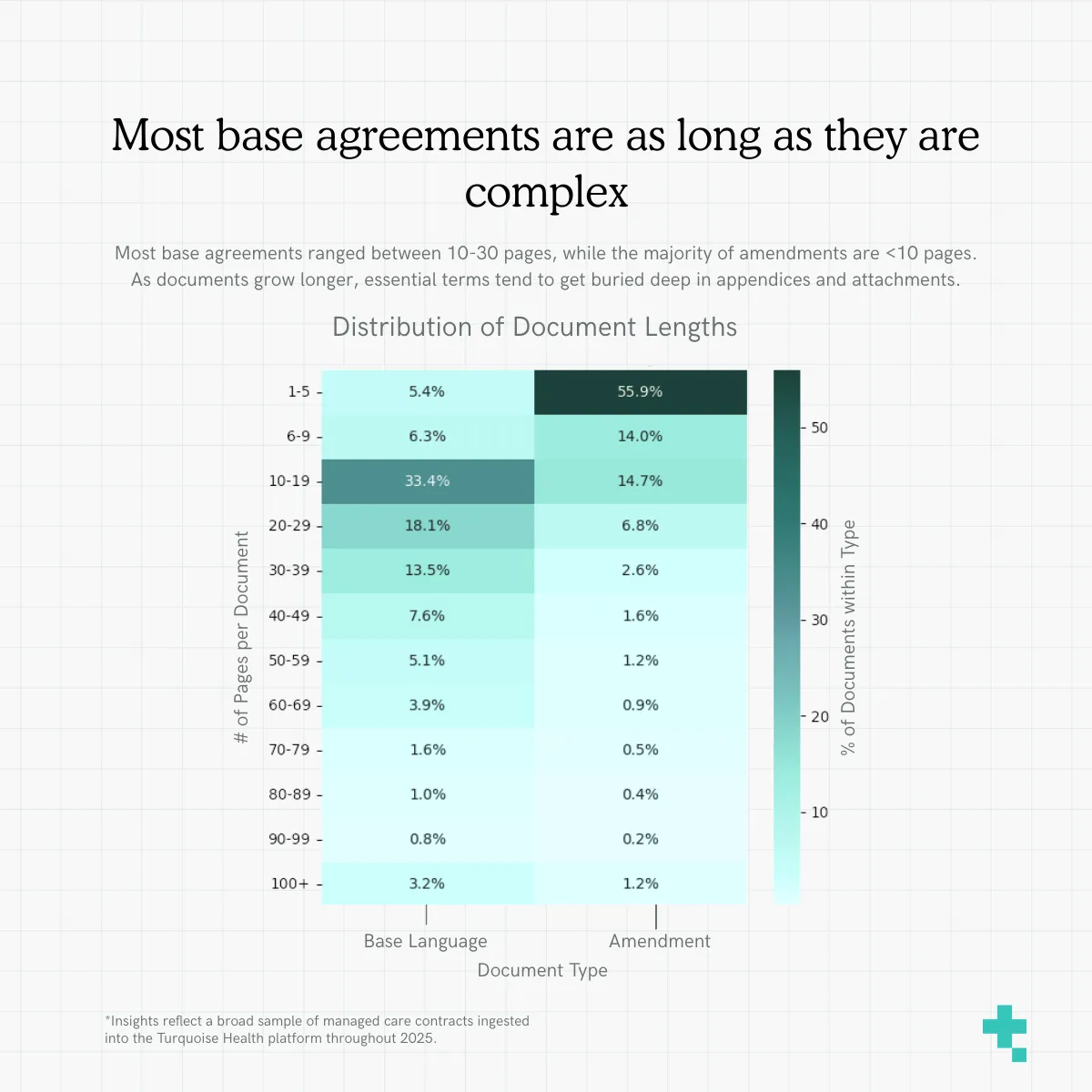
The longer the document, the higher the likelihood that key terms like appeals windows or reimbursement methodologies are buried deep in appendices or scattered across attachments. Large documents magnify the operational risk of missing something important simply because it’s too hard to find. Layer always-updating payer policies on top of these lengthy terms and you’ve got one heck of a juggling act. We’ve found this particular problem to be the best candidate for AI-applications, but more on that in a bit.
Drawer 5: The Terms
While reimbursement rates often get the most attention (guilty as charged), it’s the administrative timelines (such as the rules for filing and appealing claims) that drive the bulk of day-to-day friction between providers and payers. On its face, claims filing deadlines and appeal windows seem like a banal, practical feature of contracting. But if you’re in the know, then you know these terms are the rock and hard place between which both parties live. Taking a deeper look at which terms precisely drive that friction, we can see that this friction isn’t exclusively adversarial, it’s inherited thanks to decades-old base agreements and ways of doing business.
The majority of claims filing limits are 180 days
The variation in claims filing limits is a clear indicator of how inconsistent administrative terms can be.
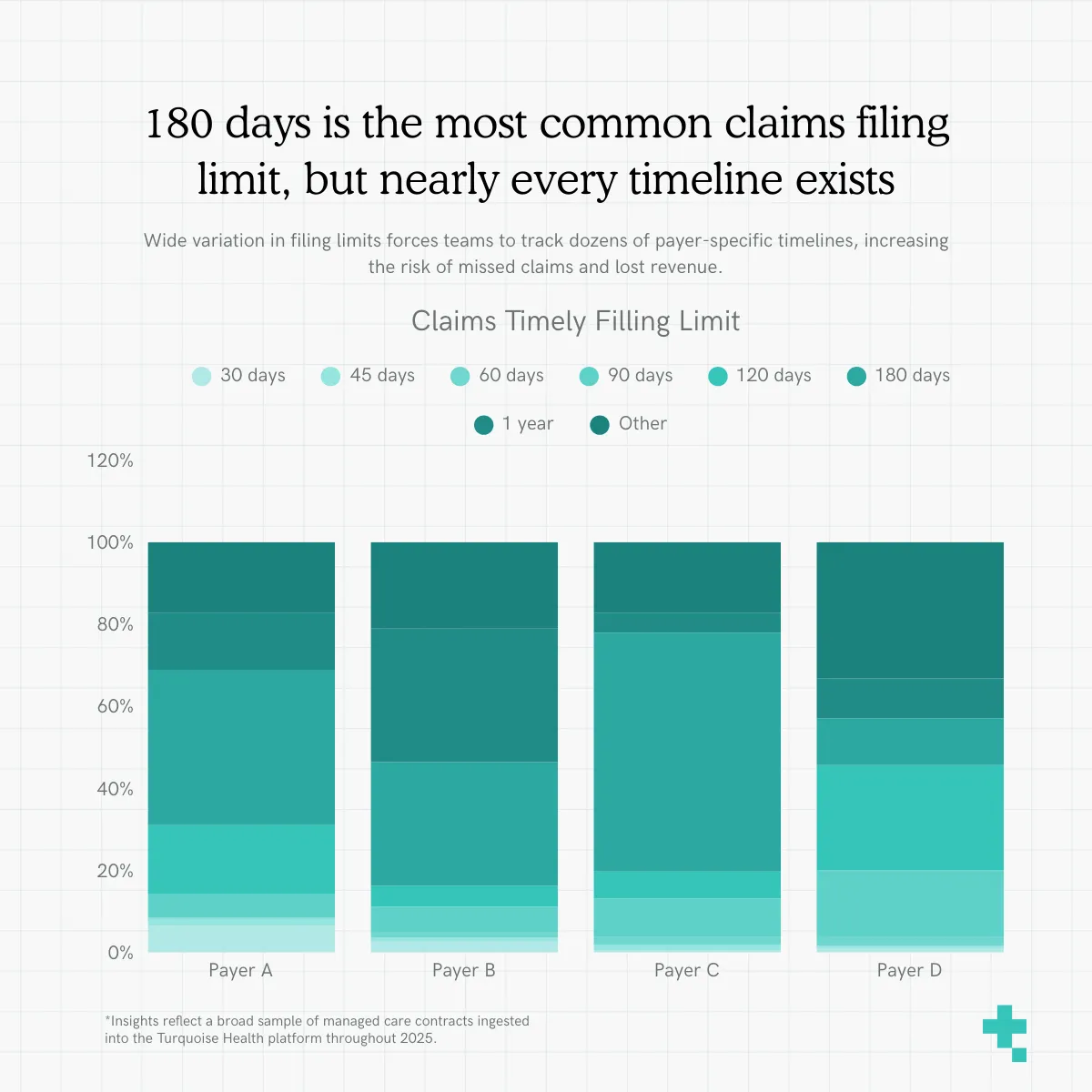
Filing windows ranged from as short as 30 days to over a year, with nearly every increment represented in between. This level of variability creates real operational risk: revenue teams must perfectly track dozens of payer-specific timelines, and a single missed filing window can turn an otherwise valid claim into permanent revenue loss.
Appeal windows ranged from 15 days to 12+ months
Appeal submission deadlines showed the same level of inconsistency as filing limits, underscoring how difficult it is for teams to navigate even the most fundamental administrative rules. Appeal windows ranged from 15 days to 12+ months, with no clear standard across payers or product lines.
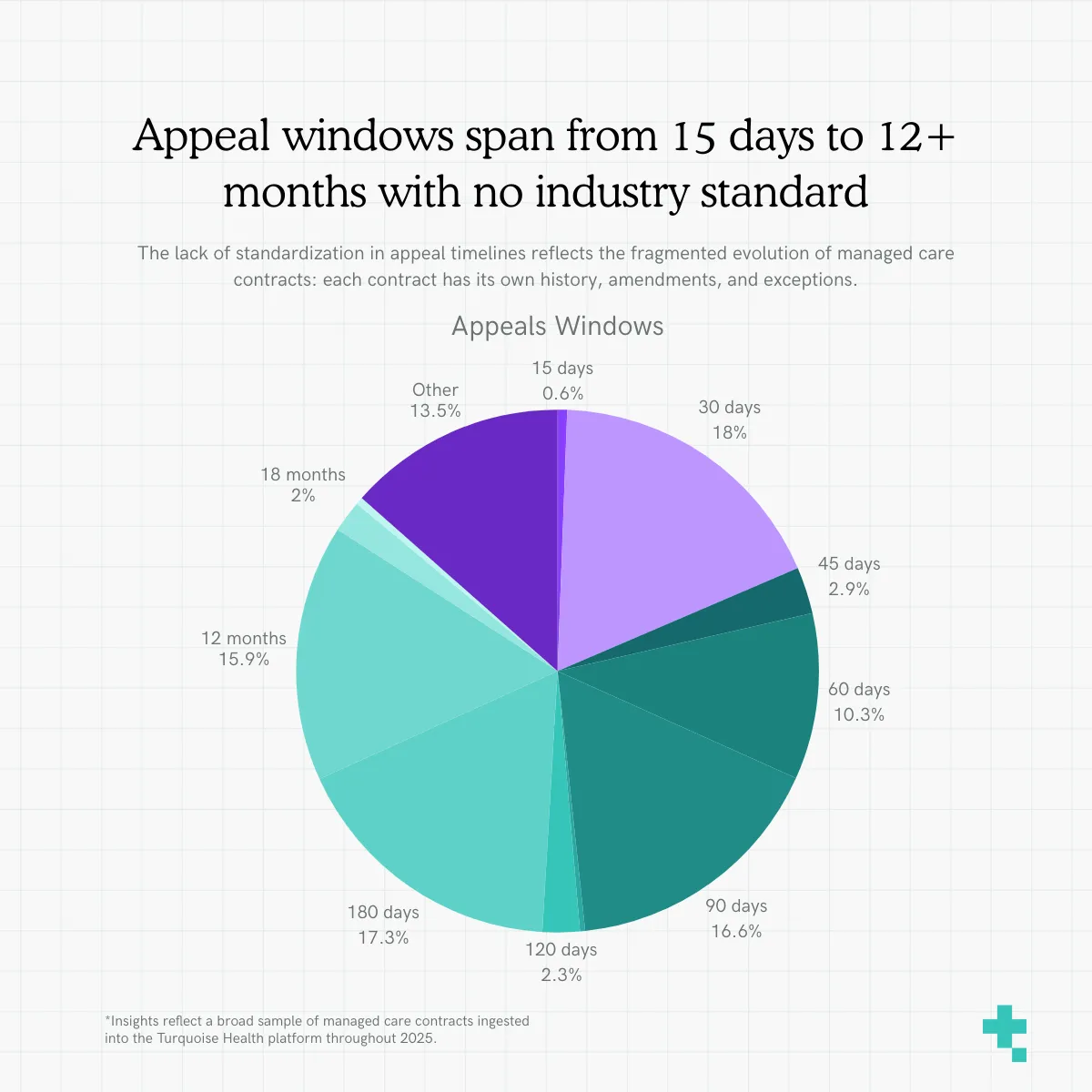
These discrepancies matter: a narrow appeal window can drastically reduce a provider’s ability to contest inaccurate payments or denials, while unclear or conflicting language increases the risk of missing deadlines altogether. What should be a simple, predictable rule instead becomes a moving target, one shaped less by design and more by the accumulated history of each individual contract. In practice, this spread of appeals windows reflects a broader fragmentation of managed care contracting as a result of non-standard contracts for siloed product lines; each contract evolves on its own timeline, often without repapering, resulting in a patchwork of rules that are challenging to manage day to day, payer to payer, claim to claim, term to term.
Drawer 6: What Questions Are Asked About Contracts?
When you combine some of our observations: agreements written 10+ years ago, repeated amendments, and unstandardized terms, what emerges are inconsistencies across every aspect of the contract. The inconsistencies we observe aren’t a sign of malicious business intent, they’re the natural byproduct of long-standing documents evolving independently across markets, payers, and service lines.
So, what’s an industry to do? Turn to the latest in tech for scalable solutions to information access and organization. The aforementioned mountains of terms, stipulations, and information contained within every contract are easily parsed, synthesized, and searched thanks to recent innovations in AI and Large Language Models (LLMs). Our AI assistant, AskTQ, allows Clear Contracts users to find answers in their contracts and payer policies, fast.
Taking a peek into the use of AskTQ, we were curious: what are users searching for?
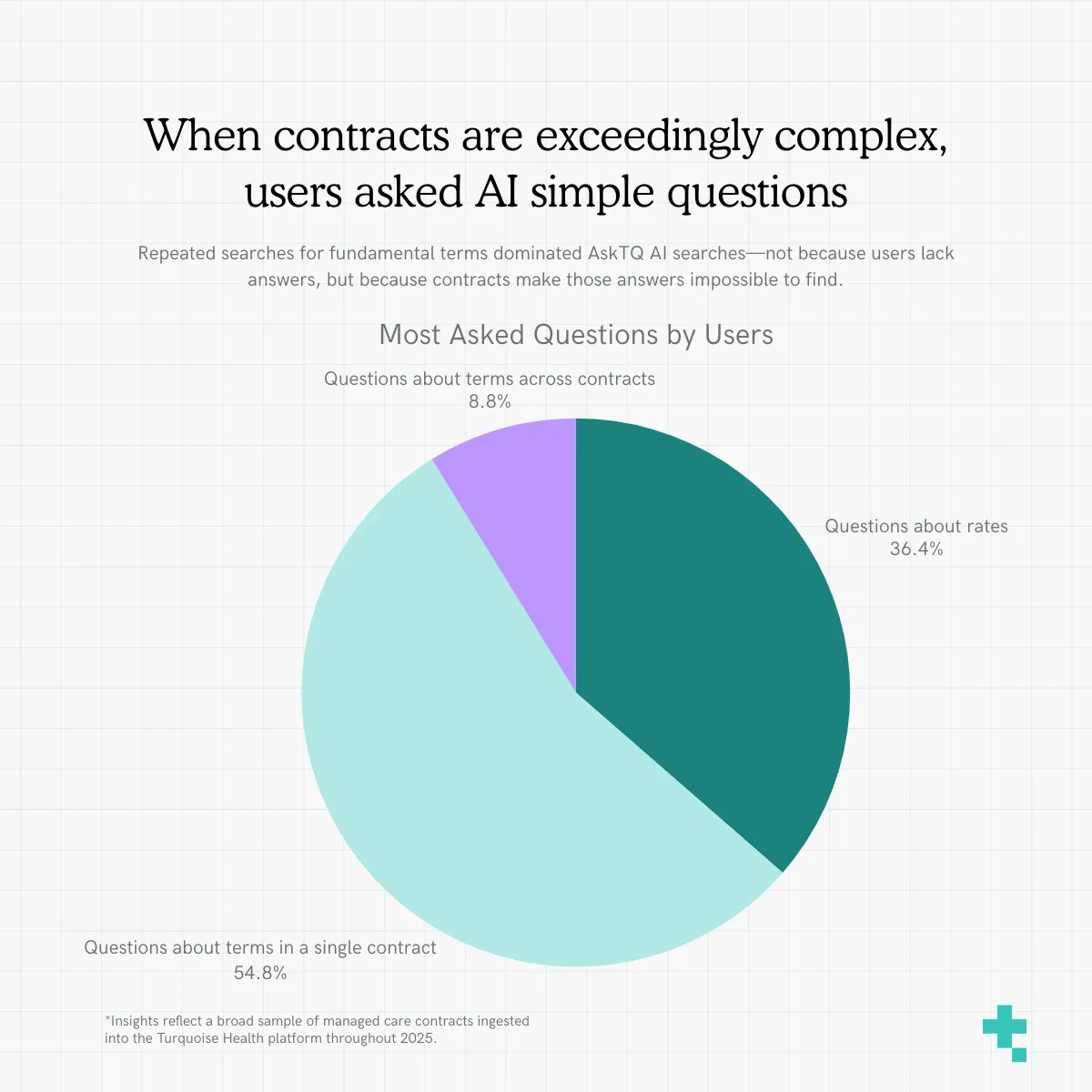
Combing thousands of questions, we found we could group questions into three main categories:
- Questions about terms across contracts (For example, “Which contracts have ____ language?”)
- Questions about terms in a single contract (For example, “Is there language about ____ in this document?”)
- Questions about rates (For example, “What is the rate for ____?”)
You might be thinking to yourself, “These are pretty basic questions. The latest in AI and this is what the people want to know?” To that we say, well, of course! The answers to those questions are buried within long, aging, non-standard and frequently amended documents. The fact that teams are repeatedly querying these basics reflects how complicated it is to unearth even the simplest of questions. In this sense, user search behavior becomes a diagnostic tool: the more often people need to ask where a critical term lives, the more it signals that contracts are not structured in a way that supports day-to-day operational clarity.
We believe when the underlying documents become easier to interpret and act upon, organizations will shift toward proactive contract management where real-time insights, transparent terms, and data-driven negotiations become the norm rather than the exception. While these findings in user behavior reaffirm the need to create operational clarity, it also shows users taking action to find the information they need, fast. Imagine what these teams are now doing with all that saved time and better access to information. Instead of reacting to denials or wasting time collecting payments, their future of managed care contracting can begin to look like one of better business relationships and hopefully, some new, never-before-answered questions.
Maybe the villain is the complexity, not your business partner
If this year inside the filing cabinet taught us anything, it’s that the contracts we ingested in 2025 weren’t legal weapons wielded by business partners both ways; they were simply the layered, aging, ever-expanding products of nuanced and complex business relationships.
When things aren’t working as well as they could, people often look for another person to blame. The long-standing narrative in healthcare administration is Everything Is Bad Because Of [Insert respective business partner here]. They’re the sole cause of confusion and strife! But looking across all these digital drawers, the picture that emerges is one of busy, complicated collaboration, not one-sided mayhem. Payers and providers are doing their best to operate with documents that were never designed to stay perfectly aligned with modern care, modern technology, or modern expectations. Add in inflation, COVID, and the overall rising cost of care - complicated documents become stages for high-stakes, bureaucratic tragedies. Everyone’s confused and no one leaves happy. While it might be easier to blame your business partner, the systemic villain of this story isn’t them, it's the complexity you both suffer and benefit from.
The road ahead isn’t one of finding more clever, nuanced tactics than your opponent. It’s to simplify complexity by giving teams the clarity, structure, and visibility needed to work confidently within the complexity they’ve inherited (and maybe standardize a thing …or two).
As we close out this Year in Observations, we are, as always, courageously optimistic. The more we digitize these filing cabinets and integrate technology, the more operational clarity teams gain. And the more clarity teams gain, the better payer<>provider relationships perform. Not because the people changed (though we’ll need some of that too) but because the paperwork finally did.
We hope you’ve enjoyed this Year in Observations as much as we have! See you in 2026 ✌️
What did you observe about your own contracts this year? We’d love to know! If you’d like to learn more about our provider- and payer-focused contracting solution, take this self-guided demo or shoot us a message.
See inside the black box
Traceable data, unified workflows, and total transparency
Related resources
Learn, listen, and watch the latest on price transparency.
CMS’ new guidance puts stop loss on center stage
Celebrating official guidance on how to encode these complex terms into MRFs