Authors
41M of 96M abandoned prescriptions in 2024 were at <$10 patient OOP. This suggests even when prescriptions are genuinely affordable, patients still abandon them. Deeper barriers are at play, including cost uncertainty.
When patients don’t know how much a drug will cost, they look for it and (more than likely) they’re using AI to search on their behalf. ChatGPT recently published a study reporting “1.6M-1.9M messages about health insurance sent weekly [by users].” These questions spanned the gamut of healthcare, “including [questions] for comparing plans, understanding prices, handling claims and billing, eligibility and enrollment, and coverage and cost-sharing details.”
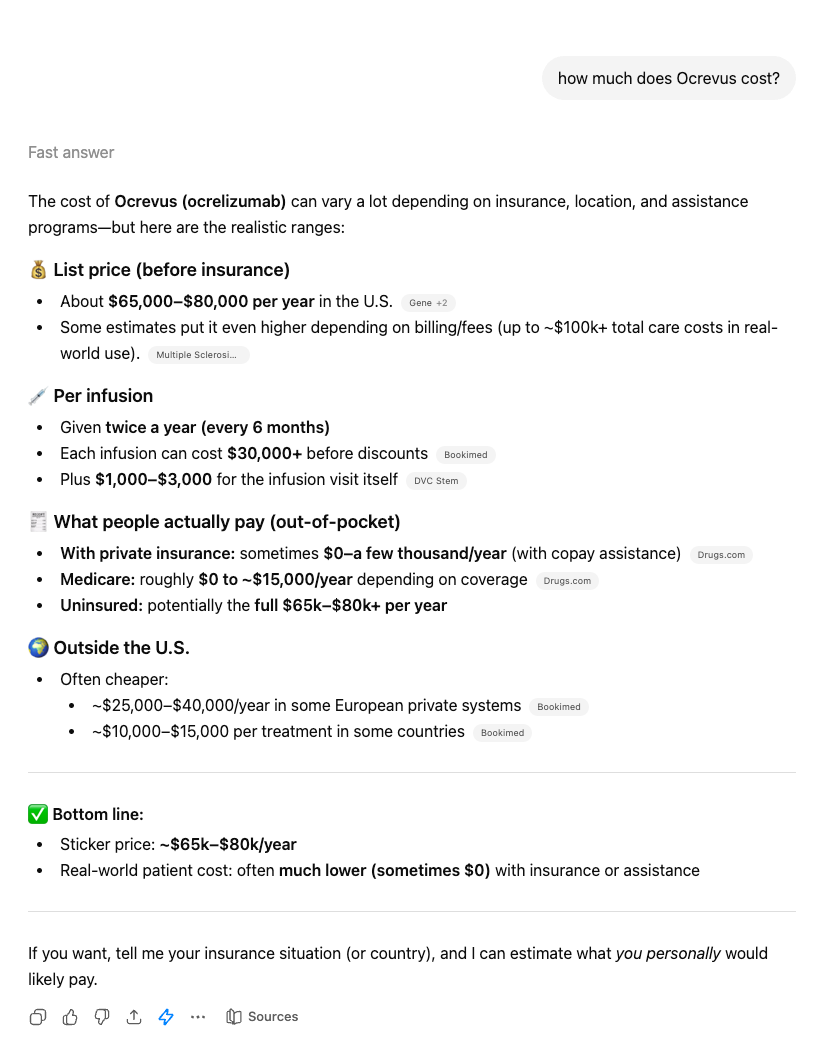
If a patient were to ask ChatGPT, “What does Ocrevus cost?” Here’s what ChatGPT will tell them: first, it will say it’s “searching the internet,” then it’ll say “List price (before insurance) About $65,000–$80,000 per year in the U.S. Some estimates put it even higher depending on billing/fees ” along with citation links to costs reported by news outlets. In this case, Multiple Sclerosis News Today, Bookimed, and Drugs.com. “The bottom line,” ChatGPT says, “With private insurance: sometimes $0–a few thousand/year (with copay assistance)."
If you ask the same question with slight semantic variation, ChatGPT will give you entirely different answers. “Is Ocrevus expensive” yields unique results totally different from our original “How much does Ocrevus cost me.” Not only is every user walking away with a different idea of price for the same drug, they still do not have an answer to what the drug will cost them uniquely. They're also leaving with information on drugs ChatGPT suggests without the right context.
Those who understand how drug pricing works know this is an over simplification of what a drug might cost. The patient’s responsibility is dependent on multiple factors like the place of service and their insurance. But the average patient doesn’t know that. A recent study found that roughly 80% of users followed faulty AI advice without question. Couple that with the knowledge that only 12% of U.S. adults possess proficient health literacy and the conclusion is clear: in the absence of an upfront price, AI now controls the cost narrative of your drug, not you.
The cost conversation has always happened without you
For decades, that’s been okay. The industry wasn’t positioned to educate and inform patients on what their out-of-pocket would be. That burden fell to others in the chain. As a result, patient access infrastructure created systems that fostered reactive cost discussions designed to meet the patient after uncertainty set in, not before. This worked prior to price transparency entering the healthcare industry. Not anymore.
In the era of price transparency, patients want to know prices upfront. Their expectations of the healthcare transaction have changed to mirror the kind of consumer behavior we expect in every other industry. Data supports this, a recent study from Surescripts showed first-fill abandonment drops 50-70% when real-time benefit information is surfaced at the point of prescribing. The cost itself no longer drives abandonment. In 2026, it’s cost uncertainty—simply not knowing the price, regardless of what that price is—that drives abandonment. If giving prices upfront was once the risk, the tables have turned. Now, it’s risky not to.
You can beat AI to the cost conversation with one necessary shift
It’s time to move from reactive to proactive patient access strategy. The manufacturers who have internalized this shift are starting to ask themselves an important question: not "Who should own the cost conversation" but "How do we own it." They recognize reactive patient access won’t work anymore. Healthcare trust has dropped from 71.5% to 40.1% in the past four years. Patients who distrust the system are now willing and ready to self-advocate. A manufacturer who proactively answers the cost question upfront becomes the most trusted entity in that patient's treatment decision because they gave the patient the one thing the rest of the system wouldn't: a real number they can use.
That's the difference between what AI is giving patients and what they actually need: a real number, personalized to their unique OOP. A proactive patient access strategy is designed to close this gap. This is no longer a patient services conversation, it's commercial strategy. The manufacturers who treat it that way are the ones who will own their cost narrative.
Global manufacturers are already making the shift to proactive patient access
The kind of proactive cost strategies that would have once felt impossible are now possible with continued advances in applications of price transparency data. Together, Turquoise and top 10 global manufacturers have built a cost estimator tool that takes price transparency data from behind-the-scenes decision-making by enterprise entities to directly surfacing prices to key decision-making points for the patient: the point post prescription. Using negotiated rate data as the foundation, then layering on capability to create episodic estimates and perform real-time eligibility checks, we are able to deliver patient-specific out-of-pocket estimates in real time, accounting for their insurance, their site of care, and the full episode cost.
While this approach is new, it isn’t novel. You can bring the same approach to your organization by prioritizing proactive patient access strategies. Chris O'Dell, President of Turquoise, and our global drug manufacturer partner are presenting a detailed look at this new approach at Asembia on April 27 during our session, “Cost Certainty as Catalyst: How Upfront Pricing for Patients Increases Access for Specialty Therapies.” They’ll cover the exact methods and walk you through how you can start owning your own cost narratives. Come see how they’re doing it.
Rates rates varied by as much as 10x ASP in our new report
We analyzed 17 medical benefit drugs across 4 therapeutic areas to find out what hospitals and payers are actually paying. Want to know?
Related resources
Learn, listen, and watch the latest on price transparency.
CMS’ new guidance puts stop loss on center stage
Celebrating official guidance on how to encode these complex terms into MRFs