Authors
On July 15, CMS released a new proposed rule that included a section on hospital price transparency. We shared some immediate thoughts on LinkedIn shortly after the proposed rule dropped and, as promised, wanted to go into more details after a few more reads and a pot of coffee.
If the proposed rule is finalized as written, the requirements would go into effect on 1/1/2026.
Specifics of the proposed requirements
Net new proposed definitions
- Tenth (10th) percentile allowed amount - the 10th percentile of the total allowed amounts the hospital has historically received from a third party payer for an item or service for a time period no longer than the 12 months prior to posting the machine-readable file. Should the calculated percentile fall between two observed allowed amounts, the 10th percentile allowed amount is the next highest observed value.
- Median allowed amount - the median of the total allowed amounts the hospital has historically received from a third party payer for an item or service for a time period no longer than the 12 months prior to posting the machine-readable file. Should the calculated median fall between two observed allowed amounts, the median allowed amount is the next highest observed value.
- Ninetieth (90th) percentile allowed amount - the 90th percentile of total allowed amounts the hospital has historically received from a third party payer for an item or service for a time period no longer than the 12 months prior to posting the machine-readable file. Should the calculated percentile fall between two observed allowed amounts, the 90th percentile allowed amount is the next highest observed value.
If the proposed rule passes as written, these new definitions would remove the requirement for hospitals to encode the estimated allowed amount (EAA). The respective percentile and median allowed amounts would fill the gap left if EAAs are removed.
Net new proposed requirements
- Alongside disclosure of the 10th percentile, median, and 90th percentile allowed amounts in machine-readable files (MRFs) when standard charges are based on percentages or algorithms, hospitals must include the count of allowed amounts.
- Hospitals should use EDI 835 transaction remittance advice (ERA) transaction data to calculate and encode these values.
Specifically, "If the negotiated percentage or algorithm associated with the allowed amounts was only used for a portion of the 12-month time period prior to posting the MRF, the hospital would encode the median and percentile allowed amounts from the EDI 835 ERA transaction data for the portion of time that the percentage or algorithm was used.
If the negotiated percentage or algorithm associated with the allowed amounts was used for the entire 12-month time period prior to posting the MRF, the hospital would encode the median and percentile allowed amount from the EDI 835 ERA transaction data for the entire 12-month time period prior to posting the MRF.
A hospital may therefore need to use different lookback periods to calculate the allowed amounts for each payer, depending on when a contract was negotiated."
Claims that paid $0 ("zero-dollar claims") must be excluded from calculations and total claim count.
- Update the attestation language hospitals must include in the MRF and to require hospitals to encode the name of the chief executive officer, president or senior hospital official designated to oversee the encoding of true, accurate, and complete data in the MRF.
Specifically, the following language is proposed: "The hospital has included all applicable standard charge information in accordance with the requirements of § 180.50, and the information encoded is true, accurate, and complete as of the date in the file. The hospital has included all payer-specific negotiated charges in dollars that can be expressed as a dollar amount. For payer-specific negotiated charges that cannot be expressed as a dollar amount in the machine-readable file or not knowable in advance, the hospital attests that the payer-specific negotiated charge is based on a contractual algorithm, percentage or formula that precludes the provision of a dollar amount and has provided all necessary information available to the hospital for the public to be able to derive the dollar amount, including, but not limited to, the specific fee schedule or components referenced in such percentage, algorithm or formula."
- Revisions that would require hospitals to encode in a newly created general data element in the MRF their Type 2 (organizational) National Provider Identifier(s) (NPI).
Specifically, "any Type 2 NPI(s) that has a primary taxonomy code starting with ‘28’ (indicating hospital) or ‘27’ (indicating hospital unit) and that is active as of the date of the most recent update to the standard charge information.”
- Propose to allow hospitals, under certain circumstances, the opportunity to have the amount of a Civil Monetary Penalty (CMP) reduced by 35% where the hospital waives its right to an Administrative Law Judge (ALJ) hearings.
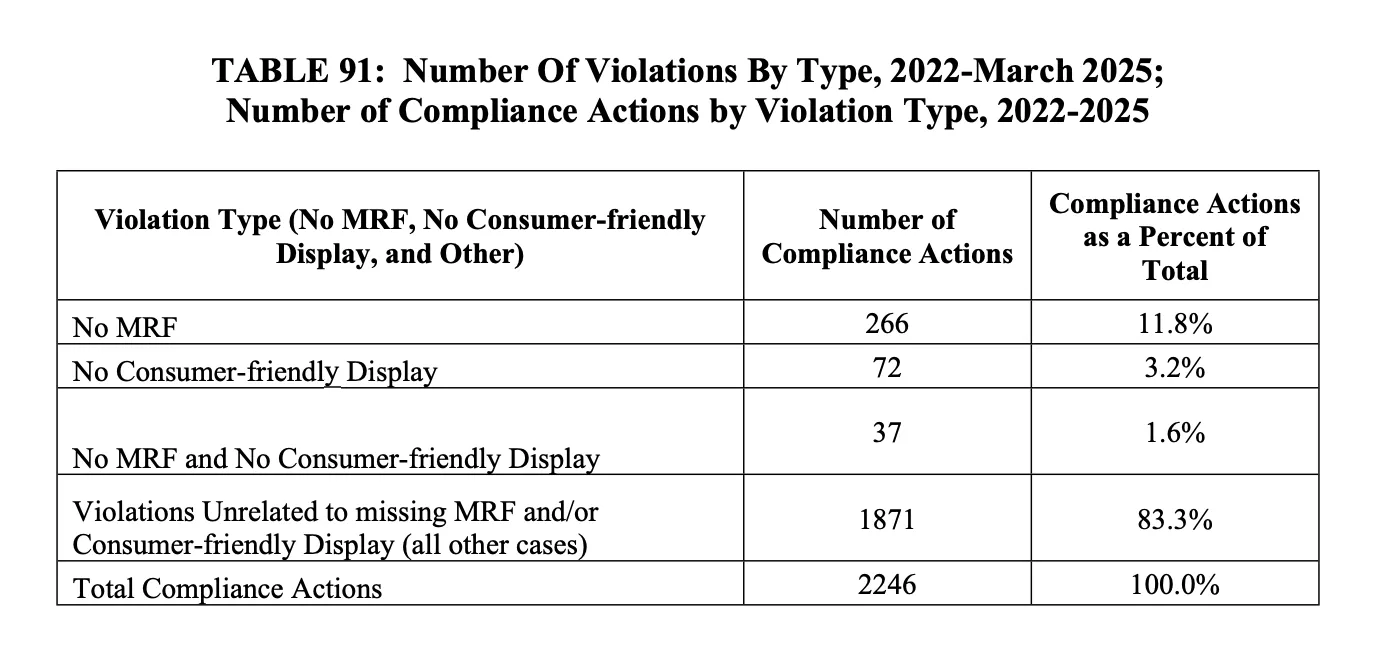
CMS notes that of the 27 CMPs issued to date, 20 hospitals have appealed their CMPs to an ALJ. Other enforcement programs offer a reduction in CMP if the entity waives its appeal rights, and CMS is now introducing the same offer to HPT. However, if a hospital remains noncomplaint after paying its 35% reduced CMP and subsequently receives a second CMP, that reduction is no longer available.
Table 91 within the proposed rule shows a summary of the compliance actions by type as of March 2025:
Themes within the proposed rule
Overall, the proposed rule seeks to build on both hospital price transparency (HPT) final rules that went into effect on 1/1/2021 and 1/1/2024, respectively. Our post yesterday goes into more details on our perspective of what this means within the price transparency landscape, but overall, CMS appears to be doubling down on a few specific areas:
- increased precision
There are a number of required elements that were somewhat of a Choose Your Own Adventure on the prior final rules. No longer. For example, this proposed rule notes specifically that "the total allowed amounts the hospital has historically received from a third party payer for an item or service for a time period no longer than the 12 months prior to posting the MRF." It also comments about how to determine the median amount in scenarios where the calculation is based on an even number of claims. CMS is getting in the weeds for the sake of increased granularity, accuracy, and ability to compare prices across MRFs.
- increased patient utility
As I noted in our post yesterday, there's a continued push to extrapolate MRF data for patient usage and price comparison. For example, the proposed rule notes that the move to percentiles, "when combined with the other data elements, provide MRF users with a better understanding of the realistic range of standard charges." Several pages in the proposed rule talk through how a patient could utilize median pricing to better understand their out-of-pocket costs.
At Turquoise, we continue to believe the burden of downloading, parsing, and utilizing MRF data falls on innovators, providers, and health plans, and patients are most likely to gain value from the data through a patient estimate tool, good faith estimate, or advanced explanation of benefits. More on these thoughts in another post.
- Utilization has entered the conversation
If hospitals are required to include claim counts at the specificity defined above, there will be new work to be done in creating MRFs. It can be tough to strike the right balance of helpful, detailed information and information that's overly burdensome to consolidate into a singular file. Payer and plan mix has also not historically been required within the price transparency landscape, so we anticipate hospitals will be asking for further clarification and seeking to protect any confidential information they use when engaging with payers to negotiate rates.
What's Next
There is a public comment period open for 60 days on the heels of this proposed rule, and Turquoise will be writing and releasing our comment. We'll be offering additional blogs, webinars, and supporting materials in preparation for any changes to come in the new year. Drop us a note here if you'd like to learn more!
See inside the black box
Traceable data, unified workflows, and total transparency
Related resources
Learn, listen, and watch the latest on price transparency.
CMS’ new guidance puts stop loss on center stage
Celebrating official guidance on how to encode these complex terms into MRFs